
With the eased CDC guidelines on mask-wearing for those vaccinated, the lifting of mandates and safety restrictions have varied significantly. Public health authorities and individuals have speculated on the timeline for a “return to normal” and what that entails: how to reopen, the adjustment to social situations, and overall experiences for this transition. Much like this moment, people in 1918-19 faced similar questions as the influenza/pneumonia crisis subsided.
From 1918 through 1919, influenza infected at least one-third of the world, causing more than fifty million deaths, with over 675,000 in the U.S. Despite its name, “Spanish Flu” likely emerged in Haskell County, Kansas in March 1918. This deadly influenza and pneumonia combination first appeared at Camp Funston and the nearby Haskell Institute – a boarding high school for indigenous students. As war raged on in Europe, domestic outbreaks of the virus continued throughout April and May, receiving very little media coverage. To most Americans, the “Spanish Flu” seemed to begin in the summer, as newspapers told of rising cases in Asia, Germany, Spain, England, and other countries. When the flu returned to U.S. soil in September, notably at Fort Devens, Massachusetts, it was perceived as the first American wave. As outbreaks spread across cities and states, its news coverage competed with and sometimes paralleled the overseas battles.
Surgeon General Rupert Blue and the U.S. Public Health Service periodically put out information and guidelines on influenza – distributed through local and national newspapers. Similar to the COVID-19 pandemic, approaches and restrictions varied geographically.With only print media, content was limited to the broad scope of the national papers or nearby outbreaks in local newspapers. In other words, people knew little about what was going on outside of their own communities.
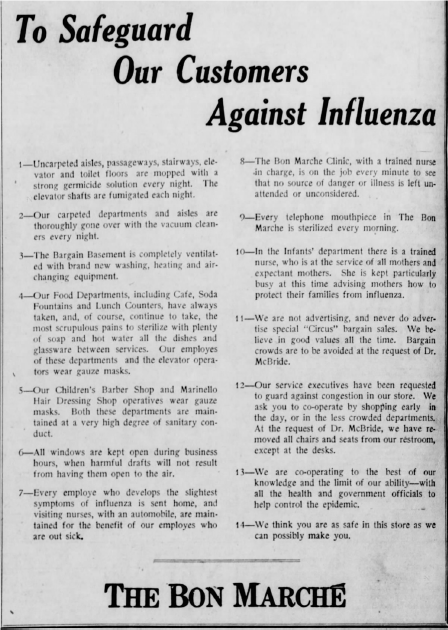
As cases rose, most towns and cities closed theaters, pool halls, and other businesses, banned dances, concerts and gatherings, and discouraged crowding in public spaces. But even this was inconsistent. Minneapolis, Minnesota closed down. Across the river, the city of St. Paul stayed open. Responses across schools also diverged, as school boards held special meetings, debating the best way to proceed. According to Alexandra Stern, Martin Cetron, and Howard Markel, most schools closed for periods up to fifteen weeks. However, Chicago, New York, and New Haven were among the cities that remained open, using medical inspection and individual quarantine to reduce transmission. Businesses that remained open marketed their adherence to safety protocol. At the end of October in 1918, Seattle’s Bon Marché department store took out full-page ads to lay out precautions taken against influenza, which included masks on the salon employees, the removal of chairs in restrooms, and a trained nurse on staff in the infants’ department “advising mothers how to protect their families from influenza.”
After the Surgeon General recommended mask-wearing in September 1918, Red Cross volunteers across the country produced identical gauze face coverings. Mask requirements were inconsistent by town. Boulder Springs, Colorado fined $100 to “any one caught not wearing a facial adornment in the form of a mask” as reported in The Anaconda Standard local newspaper. Yet in an Indiana town, children at school were exempt from mask-wearing. Private businesses also mandated masks. For example, Lima, Ohio’s Hotel Norval Domino Room advertised music and dancing in the local paper, stating, “Flu masks required.” While most hospitals required masks, Brooklyn’s Kings County Hospital banned employees from wearing them, even when cases rose among its nurses and doctors.
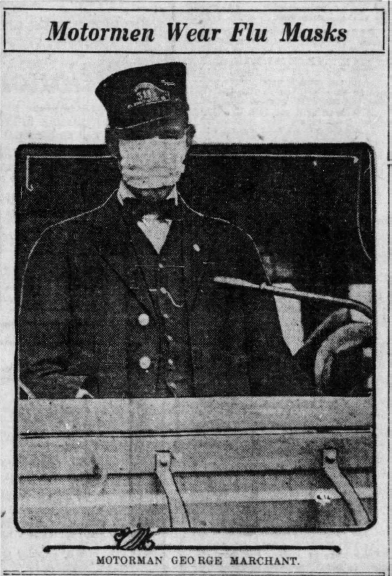
Concerns about transmission for mass transportation prompted epidemic rules for streetcars. Seattle staggered business hours to prevent overcrowding on streetcars required one-third of the windows to be open, enforced by police surveillance. In Portland, all streetcar windows had to be removed for additional ventilation. Children were altogether prohibited from riding on streetcars in Topeka, Kansas until the ban was lifted in February 1919. At Camp Gordon, Georgia, roads were sprayed with “a special antiseptic oil” to reduce the spread of germs through dust. Other rules addressed the sick and dying. New York City passed a law requiring landlords to provide heat of at least 68 degrees. Upstate, influenza victims had to be buried within twenty-four hours of death.
The reopening of society and lifting of restrictions was just as varied and confusing as it is now, if not more so. No effective vaccine existed to slow the spread, cases were inconsistently tracked, and the influx of soldiers from overseas complicated quarantine orders. “Returning to normal” in 1919 meant the reopening of society: schools, businesses, gathering places, taking part in dances and other activities that had been postponed, and gradual dissipation of fear. At the same time, for life to truly feel “normal,” soldiers had to return home and adjust to post-war life. It didn’t happen overnight.
While May 2021 does not directly parallel early 1919, the transition out of the influenza pandemic can provide insight and reassurance as to this moment. Reopening occurred over months. Just as most cities were beginning to close, Boston and others that had been hit earlier, started reopening as the end of October, with modified Halloween activities to acknowledge the somber post-epidemic tone. Across the United States, though, restrictions were temporarily halted on November, 11, 1918, as parades erupted to celebrate Armistice.

Allentown Morning Call Newspapers, Public domain, via Wikimedia Commons
Many towns then resumed restrictions, relaxing them toward the end of December or in early January, taking different approaches. News coverage on the pandemic turned optimistic before the crisis subsided. On New Year’s Day, a writer for the Lexington Herald-Leader observed, “Life is getting back into normal again, the influenza ban is about to be entirely lifted and school work to be resumed.” There’s never been uniform agreement about what to do during a pandemic or how to reopen. Public health authorities and regular people disagreed in the past and continue to do so now, with questions that resonate now: Are masks still necessary? When can sporting events resume? Will spectators be permitted? Are children safe at school? Town leaders took different approaches to relaxing quarantine and mask rules – some opening everything at once, with others easing up gradually.
In the first months of 1919, stories of enjoying the first dance after restrictions were lifted appeared next to announcements of illness and deaths. Likewise, news and social media in 2021 have juxtaposed vaccinated reunions with COVID tragedies, especially for countries that have struggled with the vaccine rollout. As society reopens, there needs to be public physical and digital spaces for remembering and mourning, and preparation for the inevitable outbreaks that will continue. Months after Seattle lifted its restrictions, the 1919 Stanley Cup Final had to be canceled on April 1st after multiple players and a team manager developed influenza, ending the series in a 2-2 tie. Assuming the Tokyo Olympics go forward, similar disruptions are likely for unvaccinated athletes and teams. Until global vaccination rates consistently high and cases decrease significantly, we too will continue to experience outbreaksand deaths.
The biggest takeaway from the “Spanish Flu” is the light at the end of the tunnel. While we need to grieve lives lost, the world has pushed through before and will do so again. Disease outbreaks have and can produce some positive changes, from improved waterways and sanitation to emergency preparedness plans. Remote learning and working, access to technology, and innovation in education are among the significant improvements that will hopefully continue forward. Lastly, the last fifteen months have sparked new interest in the history of epidemics and pandemics. The experiences and moments of COVID need to be preserved and disseminated for future generations to remember this crisis.


